Placebo Design and the Childhood Vaccine Schedule: What the Trials Were Built to Answer
Key Takeaways
- Most pre-licensure trials for schedule vaccines were designed to measure how well a product works and its short-term safety, not to detect late-emerging outcomes such as autism or chronic disease.
- All the clinical trials for vaccines on the US childhood schedule either compared a new product against another vaccine or against a carrier or adjuvant solution rather than an inert (saline) placebo, which limits what any single trial can isolate.
- Injected and swallowed aluminum behave very differently in the body, and much of the relied-upon data is from very small animal trials, which are weak points in the most-cited aluminum-safety model.
- The autism question has been pursued mainly through large observational cohort studies, which are not able to show cause-effect links. To show a link (or lack thereof), an inert-placebo randomized trial is necessary.
Medical disclaimer: Nothing in this article is medical advice. It is a discussion of clinical-trial design and published research. It does not diagnose, treat, or recommend any course of action. Decisions about vaccination belong to you and a clinician you trust.The burden of proof lies with those making the positive claim that vaccines are safe.
When a medical product is described as "placebo-controlled," most people picture a clean comparison: one group gets the product, another gets a harmless blank, and the difference between them tells you what the product did. That mental image is the standard a careful person should hold trials to. It is also worth checking against what the trials behind the childhood vaccine schedule were actually designed to measure, because the design choices shape what the results can and cannot tell us.
What a Placebo Is, and What an "Active Control" Is
A placebo, in the strict sense, is an inert substance such as sterile saline that produces no biological effect of its own. Because it is physically similar to the injection being tested, it lets researchers keep a trial "blinded," meaning neither the participant nor the evaluator knows who received what. The point of an inert control is that any difference in side effects between the two groups can be attributed to the product, not to the act of being injected.
Many vaccine trials do not use an inert control. Instead they use an "active comparator," which is another already-licensed vaccine, or a "carrier" solution that contains some of the same ingredients as the product minus the target antigen. The standard reason given is an ethics principle called equipoise: once a disease already has an effective vaccine, a review board will generally not allow children to be randomized to genuine non-protection. That logic would be reasonable for the second or third iteration of a vaccine, HOWEVER, I was shocked to learn that none of the initial versions of the vaccines on the childhood schedule in the US were tested against a true placebo. If the control group also receives the adjuvant or the carrier, the trial cannot separate effects caused by those shared ingredients, because they appear on both sides of the comparison.
What the Schedule Trials Were Designed to Measure
Pre-licensure trials are built to answer two questions: does the product produce an immune response or prevent disease, and does it cause common, near-term adverse events. They are sized and timed for those questions. They are not sized or timed to detect complex outcomes like autism, cancers and chronic disease that are diagnosed years later. A condition diagnosed well after a trial's follow-up window, in a small fraction of children, cannot be reliably detected in a study built to measure fever rates and transient rashes over a few weeks. Designing studies in this way is 100% a choice, especially for new vaccines.
So the accurate way to state it is this: the trials on the schedule were not designed to determine whether or not vaccines are linked to autism or other late-emerging chronic conditions. A study that was never built to find something cannot be cited as proof that the thing is absent, and it cannot be cited as proof that the thing is present either.
With the burden of proof lying with those making the positive claim that "vaccines are safe," I have to wonder why this billion-dollar-per-year industry can't find funding to run trials that answer everyone's questions about the potential links to autism and chronic disease. Especially as very compelling anecdotal reports of severe adverse reactions flood social media every week and more parents choose a delayed schedule or opt out entirely from the US schedule.
Did You See this Senate Hearing?
Below is a video of a senate hearing from Sept, 2025 that discusses these trial design flaws that permeate the US childhood schedule and how that has impacted public perception. This hearing includes an under oath statement by lawyer Aaron Siri, which shows proof that none of the US childhood scheduled vaccines were tested against a true placebo. This hearing is very long but worth a watch as it also covers the lack of evidence to support many of the COVID-19 era policies, propaganda, authoritarian censorship of medical professionals and other public health issues that impacted virtually everyone.
Frequently Asked Questions
Were childhood vaccines tested against a saline placebo?
None of the vaccines in the US childhood schedule were tested against a true, inert (e.g. saline) placebo control group (with the exception of the COVID-19 mRNA vaccines, which were initially designed with a true placbeo group, but were unblinded/eliminated before the end of the study). This includes the Salk Polio trial, as discussed above. The overwhelming majority of trials, especially for newer products and new versions of existing ones, used an active comparator or a carrier solution instead - which is not the same as a placebo. So the claim that "every vaccine was placebo-tested" is inaccurate.
What is the difference between an inert placebo and an active control?
An inert placebo, such as saline, has no biological effect, so any difference in outcomes can be attributed to the product. An active control is another vaccine or a solution containing shared ingredients such as the adjuvant. Active-controlled trials can show whether a new product is comparable to an old one, but they cannot isolate effects of ingredients present in both groups.
Does aluminum from vaccines build up in an infant's body?
Swallowed aluminum absorbs less than 1% (not very bioavailable), whereas injected aluminum bypasses the gut and is absorbed at a much higher rate by comparison. These two methods of exposure are very different and should not be used interchangeably (in my opinion). Modeling studies estimate the body burden and compare it to a safety benchmark, but those benchmarks are derived largely from oral-exposure data and animals, which is one reason the modeling is contested. Several studies show that heavy metals in vaccines that are injected can be absorbed into the tissues and not excreted (e.g. this study that tested thimerosal/mercury-based preservative on monkeys: https://pmc.ncbi.nlm.nih.gov/articles/PMC1280342/). This article does not make a health claim either way, but I do think we need to demand trials that are designed to answer these kinds of questions.
Were the vaccine trials designed to detect autism?
No. Pre-licensure trials are built to measure efficacy and short-term safety, not conditions like autism which are usually diagnosed years later. If a study were designed to detect conditions like autism it would include an inert placebo group so that we could compare results between those who received the vaccine and those who did not receive any of the vaccine's active ingredients. It means the trials cannot be used as direct evidence for or against such a link. Many of the existing trials compare a vaccine to a control that contains active ingredients (e.g. gardasil 9 being tested against gardasil 4 - both groups contain formaldehyde, aluminum, polysorbate-80 etc. With both groups containing active ingredients, we don't have a clean comparison that shows the relative safety of vaccinated vs unvaccinated. Gardasil 4 was also never tested against a true placebo either.
What did the large Danish studies actually find?
Unsurprisingly, The 2002 and 2019 Danish cohort studies of the MMR vaccine which were not designed to assess links to autism, did not find an association with autism. They are observational rather than inert-placebo randomized trials, a distinction worth keeping in view when judging how conclusive they are.
Why aren't more inert-placebo vaccine trials run?
The usual reason given is ethics: once an effective vaccine exists, review boards resist including a placebo group because then some would not get a potentially life-saving treatment. The issue I have with this is that even the original studies, before any other treatment is available (and thus no ethics issues), did not include a true placebo group. In 2025, regulators signaled a move toward requiring inert-placebo trials for new vaccines, however we have not seen any real movement on this as of June 2026. None of the vaccines given today on the US childhood schedule (aside from COVID-19 mRNA shots, which did not remain unblinded) were tested against true inert placebo controls.
Did the Salk polio trial use saline?
The primary-source record (the Francis Report which describes the Salk polio trial design) indicates the randomized control group received the culture medium used to grow the vaccine, rather than plain, inert saline. It functioned as a blinded control but was not inert. The salk polio trials' control group was given mixture m199 which is a combo of 60+ ingredients and included an antibiotic and red dye. Since this mixture was not inert, it's not a true placebo.
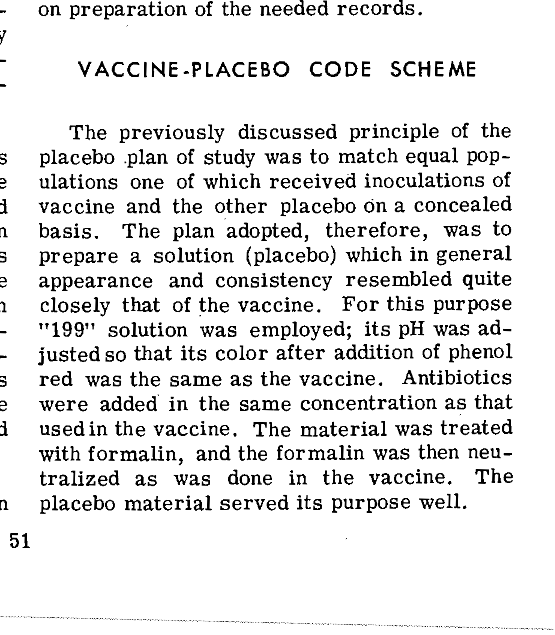
Francis report covering the study design of the Salk Polio Trials. Pg 51 documents mixture 199 was used as placebo, which is not inert. Click here to read the full PDF.
Sources & Further Reading
https://www.cdc.gov/acip/downloads/slides-2025-12-04-05/01-siri-child-imz-schedule-508.pdf - how has the childhood vaccine schedule evolved over the decades?
https://www.hsgac.senate.gov/wp-content/uploads/Siri-Testimony.pdf - transcript of Aaron Siri’s senate testimony (full hearing video embedded above)
https://pathwaystofamilywellness.org/informed-choice/danish-study-on-1-2-million-children-settles-the-vaccine-autism-debate.html - another site’s review of the danish study