
High Cholesterol? Check Thyroid Levels
The Hidden Link Between
High Cholesterol and Your Thyroid
(And Why Statins May Not Be the Answer)
If you’ve ever been told you have "high" cholesterol, your doctor's first reflex might be to write a prescription for a statin. However, standard medical care actually dictates that doctors should rule out secondary causes of high cholesterol first, and the most common culprit is an underactive thyroid (AKA hypothyroidism).
It’s my philosophy that we should always do our best to find the root cause of health issues rather than just suppressing symptoms with drugs or herbs. Let’s explore the strong connection between your thyroid, your cholesterol, and the controversial role of statin medications.
Common Symptoms of Low Thyroid (Hypothyroidism)
Because thyroid hormone regulates the metabolism of nearly every cell in the body, a deficiency can cause a wide array of systemic issues. Below is a comprehensive list compiled from standard medical organizations (CDC/NIH) as well as the pioneering clinical observations of Dr. Broda Barnes and Dr. Ray Peat:
Metabolic & Systemic
- Low Waking Temperature: Consistently waking up with a basal body temperature below 97.8°F (Barnes).
- Cold Intolerance: Chronically freezing hands and feet, or feeling cold when others are comfortable (CDC/NIH).
- Unexplained Weight Gain: A sluggish metabolism making it incredibly difficult to lose weight despite a caloric deficit (CDC/NIH).
- High Cholesterol: Due to the body's slowed ability to convert cholesterol into protective steroid hormones and bile acids (Peat/NIH).
- Slow Pulse: A resting heart rate that is notably lower than normal (Peat/NIH).
Physical & Appearance
- Dry Skin & Hair Loss: Brittle hair, dry scalp, and the classic thinning of the outer third of the eyebrows (NIH).
- Carotene Buildup (Orange Skin): A yellowish or orange tint, especially on the palms or calluses, caused by the liver's inability to convert beta-carotene into Vitamin A without adequate thyroid hormone (Peat).
- Edema (Water Retention): Puffiness and swelling, particularly around the face, eyes, or ankles, known clinically as myxedema (Peat/NIH).
- Goiter: A feeling of swelling or an visibly enlarged thyroid gland at the base of the neck (NIH).
Energy, Mood & Cognitive
- Profound Fatigue: Chronic exhaustion that isn't relieved by a full night of sleep (Barnes/NIH).
- Brain Fog: Difficulty concentrating, poor short-term memory, and feeling mentally sluggish (Barnes).
- Depression: Low mood often linked to the slowed production of crucial neurosteroids (NIH).
Digestive & Reproductive
- Constipation: Slowed gut motility and poor digestion (NIH).
- Menstrual Irregularities: Heavy, painful, or irregular periods, high prolactin levels, and potential fertility struggles (Barnes/Peat/NIH).
- Frequent Infections: A depressed immune system leading to recurring colds or infections (Barnes).
The Shifting Goalposts of "High" Cholesterol
Over the last few decades, the medical establishment has repeatedly lowered the threshold for what is considered "high" cholesterol. This has led to the mass prescription of statin drugs since now so more and more people are considered to have “high” cholesterol based on these changing numbers. But despite millions of people taking these cholesterol-lowering meds, they haven't done much in terms of drastically reducing cardiovascular disease mortality. Heart disease remains a leading killer, prompting myself and many many others to wonder if statins are really the best choice.
Here’s a timeline exploring how the cholesterol levels considered to be high have evolved over recent decades:
Pre-1984: The Statistical Average Era (>300 mg/dL Total Cholesterol)
Before the Lowering of the Goalposts
Before the 1980s, doctors primarily looked at Total Cholesterol rather than LDL or HDL fractions. Clinical laboratories generally used 300 mg/dL as the standard cut-off point for "high" cholesterol. Because the average middle-aged American had a total cholesterol level between 210 and 240 mg/dL, that range was simply considered the healthy, natural norm, and it was widely accepted that cholesterol naturally rose with age without being a disease state.
This paradigm shifted dramatically following the 1984 NIH Consensus Development Conference, which determined that the statistical "average" was actually too high. They radically lowered the threshold overnight, declaring anything over 240 mg/dL as "High Blood Cholesterol" and establishing 200 mg/dL as the new ideal limit. This shift instantly classified millions of previously "healthy" adults as patients needing treatment.
Referenced Sources:
1988 – 2004: The "Treat-to-Target" Era (<130 mg/dL lowered to <100 mg/dL)
Increasingly Strict LDL Targets
During this era, the National Cholesterol Education Program (NCEP) released the Adult Treatment Panel (ATP) guidelines. The medical consensus focused heavily on achieving specific numerical targets for Low-Density Lipoprotein (LDL) cholesterol. Over three iterations (ATP I, II, and III), these targets were consistently lowered. What started as an LDL goal of <130 mg/dL was eventually pushed down to <100 mg/dL as "optimal," with an even more aggressive <70 mg/dL target introduced for high-risk patients.
Referenced Sources:
2013: The "Risk-Based" Shift (≥7.5% Risk Score, Regardless of LDL)
Abandoning the Numbers for Risk Calculators
In a highly controversial move, the American College of Cardiology (ACC) and the American Heart Association (AHA) completely abandoned the "treat-to-target" numerical approach. Instead of treating until a patient's cholesterol hit a specific low number, they introduced a 10-year cardiovascular risk calculator. If a patient's overall calculated risk was 7.5% or higher, statins were universally recommended—regardless of what their actual LDL cholesterol levels were (unless LDL was exceptionally high at ≥190 mg/dL).
Referenced Sources:
2018 – Present: The Hybrid Approach (≥7.5% Risk + <70 mg/dL Threshold)
Blending Risk Assessment with LDL Thresholds
Realizing that specific targets still held clinical value, the ACC/AHA updated the guidelines to create a hybrid model. They retained the 2013 risk-based calculator to determine who should start taking statins, but they brought back specific LDL thresholds (such as 70 mg/dL for patients with pre-existing heart disease) to dictate when doctors should intensify treatment or add additional non-statin lipid-lowering drugs.
Referenced Sources:
And here’s a graph showing this same data:
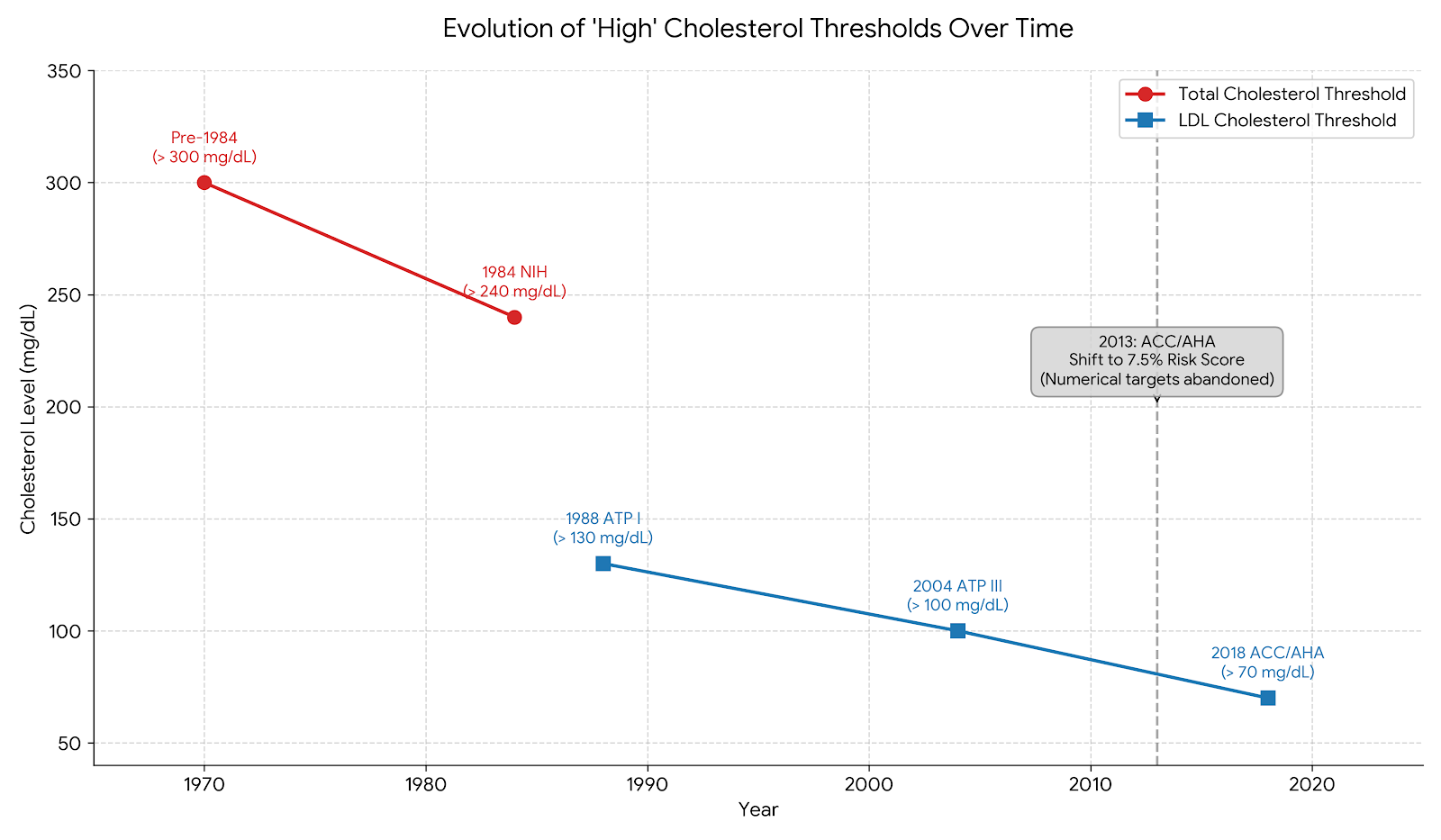
The chart traces two different measurements, as the medical focus shifted:
Total Cholesterol (Red): The focus from pre-1984 through 1984, where the standard for high cholesterol dropped dramatically from >300 mg/dL to >240 mg/dL overnight.
LDL Cholesterol (Blue): The focus from 1988 onwards, showing the steady lowering of "high" LDL from >130 mg/dL, down to >100 mg/dL, and eventually down to >70 mg/dL in 2018.
2013 Paradigm Shift: A marker notes the 2013 American College of Cardiology (ACC) and American Heart Association (AHA) decision to momentarily abandon strictly numerical targets in favor of a 7.5% 10-year risk score calculator.
Ray Peat on the True Role of Thyroid and Cholesterol
The renowned biologist and researcher that I talk about a lot on here, Dr. Ray Peat, frequently discussed the protective nature of cholesterol in his articles and interviews. He explained that cholesterol is not a toxin or harmful substance, it’s THE essential raw material your body uses to create protective, youth-associated hormones like pregnenolone, progesterone, and DHEA.
However, your body requires active thyroid hormone to convert cholesterol into these vital steroid hormones. When your thyroid function is low, this conversion process stops. Cholesterol waiting for conversion accumulates in the blood, leading to “high” cholesterol levels.
Another thyroid specialist and doctor Broda Barnes says in his book, that at the time of his writing it that probably ~40% or more of people are hypothyroid, many of them unaware of it. To me, this may explain why so many people have high cholesterol these days.
The Dangers of Statins & the Alzheimer's Connection
Before starting a cholesterol-lowering drug, it's vital to look at the broader health picture. Once you are on a statin, there’s generally no off-ramp, and your doctor will likely recommend you keep taking it for the rest of your life. I really liked this breakdown by The Midwestern Doctor has highlighted the dangers of statin drugs, linking their widespread use to a variety of chronic diseases, including severe muscle damage, insulin resistance, and profound fatigue. Midwestern Doctor is a great follow on substack for evidence-based functional health information from someone who is a practicing MD. I refer to their articles often since most of my education is centered on biochemistry and the medicinal compounds found in herbal medicine and other alternative therapies, and less on Rx medications.
I’m including this because we are currently seeing Alzheimer's disease at an all-time high. The brain is a highly fat-dense organ, made up of roughly 60% fat, and it contains about 25% of the body's total cholesterol (myelin, which insulates the neurons of your brain is very high fat). The brain relies heavily on cholesterol to function, build synapses, and maintain memory. While the medical establishment hasn't officially proven a direct link, common sense suggests that a drug designed to chemically alter how the body metabolizes fats and drastically lower cholesterol could have severe implications for cognitive health.
How to Accurately Test Your Thyroid (The Broda Barnes Method)
While doctors typically use a TSH blood test, this doesn't always show how well thyroid hormone is actually working at the cellular level. I recently read a book by Dr. Broda Barnes, where he explains his discovery that your Basal Body Temperature (BBT) is one of the most accurate indicators of metabolic and thyroid function, and is far more accurate than the expensive blood tests we often have to beg our doctors to run.
How to test your BBT:
Get the right tool: You need a specific Basal Body Temperature (BBT) thermometer, which is highly sensitive. Regular fever thermometers are not sensitive enough.
Keep it close: Place it on your nightstand before you go to sleep.
Test immediately: The absolute key to this test is taking your temperature the exact moment you wake up. You must do this before moving, sitting up, or talking, as any activity raises your body temperature and voids the test. Note that most BBT thermometers take several minutes to get an accurate reading.
According to Dr. Barnes, consistently low waking temperatures (below 97.9 degrees) strongly suggest an underactive thyroid, regardless of what standard blood work might say.
Addressing the Root Cause of Low Thyroid
If you discover your thyroid is low, resolving it will naturally lower your cholesterol as your body begins properly converting it into hormones again. I have read a lot of the work by Ray Peat Phd, who was an endocrinologist and hormone specialist. Some of his ideas are not widely accepted by the pharma-sponsored medical establishment since they rely on dietary and lifestyle changes which are not taught in conventional medicine.
Ray argued that the body downregulates thyroid function (specifically by reducing the active thyroid hormone, T3) as a defensive adaptation to stress, toxins, or a perceived lack of energy. When the body senses danger or starvation, it slows the metabolism to conserve resources.
Just a reminder that this article is for educational purposes and is not medical advice. Please consult with your healthcare provider for advice specific to your situation. I am not a doctor.
Here is a comprehensive list of factors that contribute to thyroid suppression according to his research on the endocrine system and philosophy on naturally supporting thyroid health:
Dietary Factors
Polyunsaturated Fatty Acids (PUFAs): Liquid industrial seed oils (soybean, canola, corn, safflower, sunflower) and even fish oils (which are usually highly oxidized and pro-inflammatory after being removed from the fish) are highly toxic to the metabolism. According to Ray Peat Phd, PUFAs block the secretion of thyroid hormone from the gland, inhibit its transport in the bloodstream, and block the thyroid receptors at the cellular level.
Low-Carbohydrate Diets: The liver requires adequate glucose to convert inactive T4 into active T3. Low-carb, keto, or fasting diets as starvation signals that trigger the release of stress hormones (cortisol and adrenaline) to raise blood sugar by breaking down tissues, which profoundly suppresses the thyroid.
Excessive Estrogen & Phytoestrogens: Estrogen is a primary antagonist to the thyroid and blocks the liver's ability to convert T4 to T3. Soy products are something that I avoid because of their high concentration of plant estrogens (phytoestrogens).
Low Protein Intake: The liver needs adequate high-quality animal protein to produce the enzymes required for hormone synthesis and detoxification. Without it, thyroid function will suffer.
Amino Acid Imbalance: Eating only muscle meats provides high amounts of tryptophan and methionine, which can be inflammatory and pro-serotonin (a stress hormone according to Ray Peat). Balancing muscle meats with gelatin or collagen helps counteract this.
Goitrogenic Foods: Certain raw cruciferous vegetables (like broccoli, cabbage, cauliflower, and kale) contain goitrogens that can directly suppress the thyroid gland if eaten raw or in massive quantities.
Excessive Iodine: While necessary in trace amounts, large doses of iodine (often found in commercial iodized salt, supplements, or dough conditioners) can act as a powerful thyroid inhibitor.
Fluoride: Common in municipal tap water and toothpaste, fluoride is a potent enzyme poison that actively competes with iodine and damages the thyroid gland. Around 30% of all medications contain a covalently bonded fluorine atoms (synthetically made fluoride), which is added to help medications cross the blood-brain barrier and absorb better. The list of all meds that include a fluoride atom is very long and includes SSRI’s, Statins, antibiotics, antifungals, corticosteroids, antacids, proton pump inhibitors, and certain cancer treatments.
Lifestyle & Stress Factors
Endurance Exercise: Intense, prolonged cardiovascular exercise (like long-distance running) is a massive physical stressor. It accelerates the breakdown of thyroid hormones, forcing the body into an "adaptive hypothyroidism" to survive the stress. Endurance athletes often have a very low resting heart rate, which really is evidence of metabolic slowing, rather than superior heart health. That’s not at all saying that you shouldn’t exercise, just switch to more strength training-centered workouts instead rather than cardio.
Psychological Stress: Chronic mental stress elevates cortisol, adrenaline, and serotonin. High cortisol directly blocks the conversion of T4 to T3 and breaks down muscle tissue for energy, further slowing the metabolism.
Lack of Sunlight (and Excess Blue Light): Metabolic needs increase in cold, dark environments. Sunlight, specifically red and near-infrared wavelengths, stimulates mitochondrial respiration and supports thyroid function. Conversely, excessive exposure to artificial blue light at night acts as a biological stressor. Plenty of studies backing this up as this area of research is exploding recently. I know a lady who was able to correct her low thyroid blood test numbers just by using a red light therapy panel daily.
Sleep Deprivation: Poor sleep elevates stress hormones (cortisol and adrenaline) and increases insulin resistance, both of which actively suppress thyroid hormone production and cellular energy generation. Many sleep disorders like sleep apnea are actually linked to low thyroid hormones.
Environmental Toxins & Biological Stressors
Bacterial Endotoxin: Poor digestion or slow bowel transit allows bacteria in the intestines to overgrow and produce endotoxin (lipopolysaccharide). When this leaks into the bloodstream, it burdens the liver, spikes estrogen and serotonin, and aggressively suppresses the thyroid. (He often recommended raw carrot salads or well-cooked white button mushrooms to bind and clear these endotoxins).
Mold and Mycotoxins: While Ray did not focus exclusively on mold in the way some functional medicine practitioners do, his framework categorizes mycotoxins as severe environmental stressors. Inhaling or ingesting mold toxins heavily burdens the liver. A taxed liver cannot efficiently detoxify estrogen or convert T4 to T3, leading to systemic thyroid and metabolic suppression. Mold exposure also triggers histamine and inflammatory cascades, which raise cortisol and serotonin.
Heavy Metals: Metals like aluminum & mercury (found in seafood, supplements, dark chocolate, and silver amalgam dental fillings) and lead poison the enzymes necessary for thyroid hormone production and the crucial T4 to T3 conversion.
Pesticides and Herbicides: Many agricultural chemicals act as endocrine disruptors or xenoestrogens (estrogen mimics). By increasing the body's total estrogen burden, they inhibit thyroid function. Additionally they probably also harm the liver.
Radiation: Peat wrote extensively about how environmental radiation (ranging from excessive medical X-rays to environmental fallout) damages the sensitive tissues of the thyroid gland, increasing the risk of hypothyroidism and tumors.
Relevant Articles: Supporting Low Thyroid


HypoThyroid OTC Supplement Support
Note that if your thyroid is removed, severely damaged (like in Hashimoto’s), or dead, supplements are probably not going to replace a prescription medication. These supplements act as a gentle support, which is great for those who are mildly hypothyroid, but likely not strong enough for more severe cases. Again, none of this is medical advice, please consult with your doctor.
4. Progest-E / Progesterone (OTC)
Progest-E is often mentioned by Ray Peat, and others who follow his work online as a thyroid-supportive supplement. Progest-E is a product that blends anti-inflammatory vitamin E and natural progesterone.
Why Progesterone for Hypothyroid?
Mainstream medicine views estrogen as a vital female sex hormone necessary for bone, heart, and brain health. Ray Peat, however, fundamentally disagreed after years of research into female hormones. He argued that estrogen lowers the body's temperature, creates intracellular hypoxia (lack of oxygen in the cells), and promotes inflammation and tissue aging. Additionally, excess estrogen suppresses the thyroid gland from releasing its hormones and increases proteins in the blood that bind to thyroid hormones, making them inactive.
He recommended progesterone primarily as an estrogen antagonist. He believed that supplementing progesterone would block the toxic effects of estrogen, halt tissue degradation, and restore cellular energy.
Progesterone Dosing Schedule
For women, Ray recommended that this supplement should only be taken from ovulation through to the first day of menstruation (days ~15-28), not the whole month. For perimenopausal women, take on the same schedule, calculating when your menstrual period would be. Ray recommended for menopausal women to take the same dose every day. Again, this is for educational purposes and is not medical advice.
Pros: Estrogen dominance can bind up thyroid hormones in your blood, making them unusable. Supplementing progesterone can help balance estrogen, which indirectly frees up your natural thyroid hormones to do their job.
Cons: It is a sex hormone, not a thyroid medication. It will not cure clinical hypothyroidism, but it can support it in a roundabout way.
Side Effects: Drowsiness (it is very relaxing), changes in menstrual cycle timing, mood shifts, or bloating if the dose isn't right for your body. Progesterone also can slow down disgestion, leading to constipation.
Cost: Moderate (around $30–$40 a bottle).
Ease of Rx / Availability: No prescription needed. Readily available to order online in the US. Store in the fridge for longer shelf life.
5. Thyroid+ from Heart & Soil
This is a dietary "nose-to-tail" supplement containing freeze-dried bovine (beef) liver, kidney, and thyroid gland. I added this to the list because it’s what I currently take to support my mild hypothyroid that developed after living for several years in a house that had black mold.
Pros: It provides highly bioavailable micronutrients, vitamins, and trace minerals that support overall metabolic health. This is not a medication and requires no prescription. Food-based supplements are less likely to have contaminants from industrial processing, and are far more bioavailable than synthetics. This one is made from regeneratively-farmed, grass-fed/finished cows.
Cons: Because it is a food-based supplement, the amount of actual active thyroid hormone in each capsule is unstandardized. My experience has been that the dose feels the same from bottle to bottle, but if you ask any doctor they will tell you that the dose is unstandardized and that could cause hormone crashes.
Side Effects: Generally safe as a food-based supplement, but risks include unexpected hyperthyroid symptoms if a batch is particularly potent.
Cost: High (usually around $60–$65 per bottle).
Ease of Rx / Availability: No prescription needed. Easily ordered online in the US.
HypoThyroid Rx Treatment Options
In the interest of informing you of all of your options, you should know that there are several options for treating thyroid that require a prescription. There are pros and cons that go with each, and I think the best option will depend on your health picture.
Levothyroxine (AKA Levo, Synthroid, Tirosint, generic T4)
Levothyroxine is a synthetic version of T4, the inactive storage hormone that your body must convert into T3 (the active hormone) to use.
Pros: It has a long half-life, meaning blood levels stay very steady. It is the medical “standard of care”, meaning there is decades of data behind it.
Cons: It contains ONLY T4. Many people have poor T4-to-T3 conversion. If your body doesn't convert it well, your lab tests might look "normal," but you will still feel hypothyroid.
Side Effects: Generally minimal unless the dose is too high (causing anxiety, heart palpitations, insomnia) or too low (causing continued hypothyroid symptoms).
Cost: Very inexpensive (often under $10/month for the generic).
Ease of Rx: Extremely easy. Any regular doctor or endocrinologist will prescribe this without hesitation.
US Availability: Universally available at any pharmacy.
NDT (Natural Desiccated Thyroid - AKA Armour, NP Thyroid)
NDT is derived from dried porcine (pig) thyroid glands. It contains both T4 and T3, as well as trace amounts of T2 and T1.
Pros: Many patients who feel poorly or still have hypothyroid symptoms on Levothyroxine report feeling significantly better on NDT because it provides direct active T3. This may be due to the fact that the forms of thyroid hormones are more bioavailable than the synthetic versions, and contain cofactors that can help with absorption. We evolved eating animal organ meats, so this is something our bodies are evolutionarily used to dealing with.
Cons: Pigs naturally produce a higher ratio of T3 to T4 than humans do (about 4:1 in pigs vs. 14:1 in humans). This can cause a sudden spike in T3 shortly after taking it.
Side Effects: Heart palpitations or jitteriness if the T3 hits your system too fast.
Cost: Moderate (usually $15–$40/month, though brand-name Armour can be more).
Ease of Rx: Moderate. Many conventional endocrinologists dislike NDT, citing historical (though largely resolved) batch inconsistencies. However, many standard primary care doctors, osteopaths (DOs), and functional medicine doctors will prescribe it.
US Availability: Widely available, though the supply chain can occasionally experience backorders. Recently there was word of possible move by the FDA to ban NDT (article about this below) for some reason, but that seems to not be happening due to public backlash after the announcement.
Cynomel (Liothyronine / Cytomel)
Note: "Cynomel" is an international brand name that is commonly used in Mexico and Europe. In the US, this medication is known by the brand name Cytomel or the generic Liothyronine. It is basically just pure, synthetic T3 (the active hormone). Often it is prescribed as an add-on to dose alongside levothyroxine.
Pros: It provides immediate, active thyroid hormone. It is excellent for people who cannot convert T4 to T3.
Cons: T3 has a very short half-life. If you take it all at once, you might get a rush of energy followed by a crash later in the day. It often requires being split into two or three doses daily.
Side Effects: High risk of hyperthyroid symptoms (rapid heart rate, sweating, anxiety) if the dose is even slightly too high.
Cost: Generic Liothyronine is inexpensive to moderate ($10–$30/month).
Ease of Rx: Difficult with a standard doctor. Most conventional doctors hesitate to prescribe T3-only medications due to the cardiovascular risks of accidental overdosing. You usually need an endocrinologist or a functional medicine doctor.
US Availability: Readily available as Cytomel or generic Liothyronine. You cannot get the "Cynomel" brand at a US pharmacy without importing it.
Frequently Asked Questions (FAQ)
1. Why does my cholesterol go up when my thyroid is low? Your body needs adequate thyroid hormone to convert cholesterol into essential steroid hormones (like progesterone and DHEA) and bile acids. When thyroid function slows down, this conversion process stops, causing cholesterol to build up in your bloodstream.
2. What temperature indicates a low thyroid according to Broda Barnes? Dr. Barnes stated that a normal waking basal body temperature should be between 97.8°F and 98.2°F (measured under the arm for 10 minutes). Consistently waking up with a temperature below 97.8°F is a strong indicator of low thyroid function.
3. Are statin drugs the only way to lower high cholesterol? No. If your elevated cholesterol is a secondary symptom of an underactive thyroid, treating the thyroid naturally brings cholesterol levels down. Dietary adjustments, reducing systemic inflammation, and balancing minerals can also support healthy lipid metabolism without the use of statins.
4. What is the difference between Levothyroxine and NDT? Levothyroxine (Levo) is a synthetic form of T4, a storage hormone that your body must convert into active T3. Natural Desiccated Thyroid (NDT) is derived from animal thyroid glands (usually from pigs or cows) and contains a natural ratio of T4, active T3, and other trace thyroid hormones, which often mimics the human body's natural output much better.
5. Why are statins potentially dangerous for brain health? The brain contains about a quarter of the entire body's cholesterol, which it desperately needs to maintain cell membranes, build synapses, and facilitate fast communication between neurons. Statins cross the blood-brain barrier and interfere with cholesterol synthesis, which may deprive the brain of the fats it needs to prevent cognitive decline.
Fish oil supplements are often oxidized and pro-inflammatory. This article explains why omega-3s are best obtained from whole foods like eggs, sardines, and salmon instead of capsules.