
The Importance of Differential Diagnosis: Symptom Overlap in Outbreak Regions
Key Takeaways
- Acute arsenic poisoning produces a clinical profile nearly identical to Ebola, including vomiting, watery diarrhea, abdominal pain, gastrointestinal hemorrhage, vascular collapse, and hypovolemic shock.
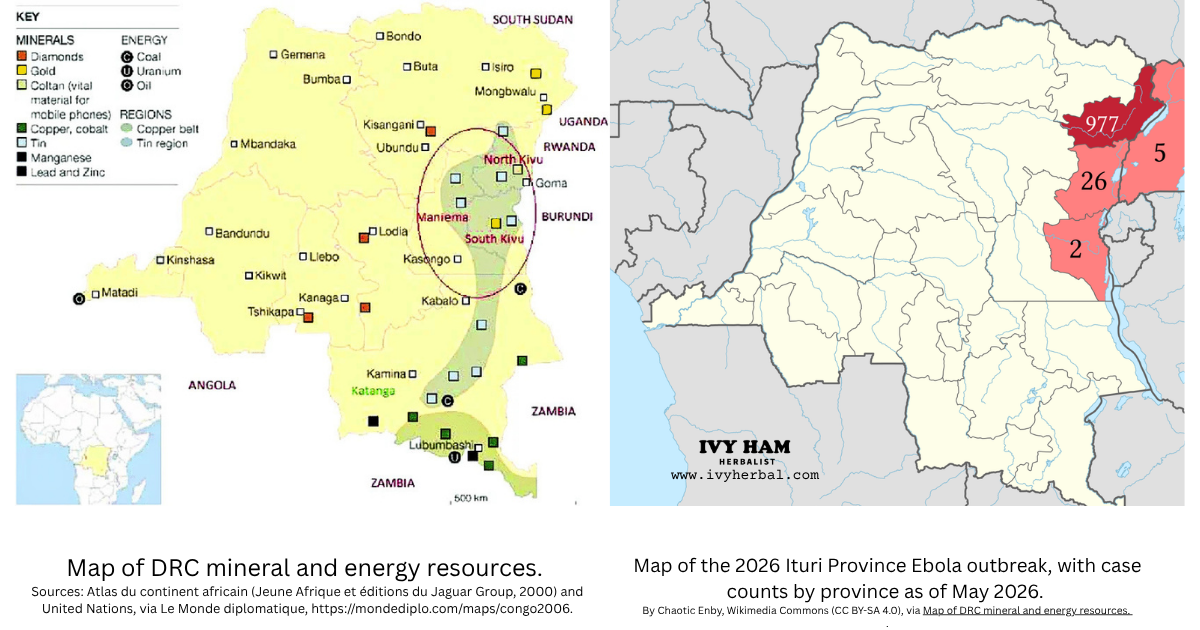
- The DRC's extensive gold, copper, and cobalt mining operations release arsenic and other heavy metals into local soil and water, making toxicity a documented environmental hazard for nearby communities.
- Outbreak diagnostics rely almost exclusively on PCR and genomic sequencing, which detect genetic material but do not establish disease causation, and arsenic testing is not part of the standard workup.
- Treatment protocols differ dramatically (supportive care for viral hemorrhagic fever versus chelation therapy for heavy metal toxicity), so a missed differential diagnosis can mean a missed antidote.
In public health, accurate diagnosis is the foundation of effective treatment. Administering the wrong clinical protocol can be fatal, which is why establishing a rigorous differential diagnosis is critical to saving human life. In the Democratic Republic of the Congo (DRC), health authorities frequently manage outbreaks of severe hemorrhagic and gastrointestinal illness. While public health responses overwhelmingly prioritize viral etiologies like the Ebola virus, it is necessary to ask whether environmental factors are being adequately evaluated before determining a root cause.

Gold & tin mine locations on the left map match ebola outbreak areas on the right map.
Symptom Overlap and Environmental Hazards
When an individual presents with sudden onset fever, severe weakness, muscle pain, abdominal pain, vomiting, watery diarrhea, vascular collapse, and hemorrhage, the immediate clinical suspicion in certain regions defaults to Ebola. However, these clinical manifestations are not exclusive to viral hemorrhagic fevers. The WHO itself acknowledges that "it can be difficult to clinically distinguish Ebola from other infectious diseases such as malaria, typhoid fever and meningitis," yet environmental toxicology rarely appears on that differential list at all.
Acute arsenic poisoning presents with a nearly identical clinical profile. According to the CDC's Agency for Toxic Substances and Disease Registry (ATSDR), acute arsenic exposure produces "nausea, vomiting, diarrhea, gastrointestinal hemorrhage, cerebral edema, tachycardia, dysrhythmias, and hypovolemic shock." A peer-reviewed clinical review of acute arsenic intoxication further notes that "hypotension, fluid and electrolyte disturbances, mental status changes, electrocardiographic abnormalities, respiratory failure and death can result." The gastrointestinal distress, systemic shock, and hemorrhagic symptoms seen in severe heavy metal toxicity mirror the symptomology currently attributed to viral outbreaks in the region.
| Symptom | Acute Arsenic Poisoning | Ebola Virus Disease |
|---|---|---|
| Sudden-onset fever | Can occur secondary to systemic toxicity, dehydration, and inflammatory response; not a defining primary feature | Hallmark early symptom; typically sudden onset, often high-grade (above 38.6°C / 101.5°F) |
| Severe weakness / fatigue | Common; caused by systemic enzyme inhibition (arsenic blocks pyruvate and succinate oxidation), dehydration, and electrolyte loss | Early and persistent; classified as part of the "dry symptom" phase preceding GI involvement |
| Muscle pain (myalgia) | Common; muscle cramps and leg cramps reported, often following the initial GI phase | Early symptom; widespread muscle and joint pain typical in first days of illness |
| Severe headache | Common, frequently accompanied by encephalopathy and mental status changes in severe acute toxicity | Hallmark; often described as severe and frontal; a recognized early diagnostic indicator |
| Abdominal pain | Hallmark feature; colicky in nature, onset within minutes to hours of ingestion | Common during symptomatic "wet" phase; often accompanies GI involvement |
| Vomiting | Hallmark; severe and persistent; results from direct toxicity to gastrointestinal epithelial cells | Hallmark; emerges as illness progresses from "dry" to "wet" symptoms |
| Watery diarrhea | Hallmark; profuse, sometimes described as "rice-water" in consistency; can contain blood with severe mucosal damage | Hallmark; can be voluminous and is a major contributor to hypovolemic shock |
| Gastrointestinal hemorrhage / unexplained bleeding | Documented; results from inflammation and necrosis of GI mucosa; can present as bloody vomit, stool, or perforation | Documented in late stages; bleeding from gums, GI tract, injection sites, and other orifices in severe cases |
| Hypotension / vascular collapse | Multiple mechanisms: decreased cardiac contractility, increased vascular permeability, diminished peripheral vascular tone | Driven by fluid loss, capillary leak, and disseminated intravascular coagulation |
| Tachycardia / cardiac dysrhythmia | Sinus tachycardia common; QT-interval prolongation and T-wave inversion documented on EKG | Common; secondary to hypovolemic shock and electrolyte disturbance |
| Mental status changes / encephalopathy | Cerebral edema reported; confusion, agitation, and altered consciousness in severe toxicity | Late-stage feature; confusion and agitation can precede coma |
| Multi-organ failure | Cardiac, hepatic, and renal involvement common in severe acute exposure; respiratory failure can occur | Impaired kidney and liver function documented; respiratory complications in advanced disease |
| Hypovolemic shock leading to death | Death from acute arsenic poisoning is most often attributed to cardiovascular collapse and hypovolemic shock | Shock from fluid loss and circulatory collapse is a leading cause of death in untreated cases |
Sources: CDC/ATSDR Arsenic Toxicity Clinical Assessment; ATSDR Medical Management Guidelines for Arsenic; PubMed: Acute Arsenic Intoxication; StatPearls: Arsenic Toxicity; WHO Ebola Disease Fact Sheet; CDC Ebola Disease Basics; Johns Hopkins Medicine: Ebola.
This overlap is highly relevant in the DRC. The region is home to extensive gold mining operations, and arsenic naturally occurs alongside gold deposits. The extraction and refinement processes frequently release toxic levels of arsenic into the surrounding soil and local water supplies. A 2022 study published in Environmental Advances documented arsenic, cadmium, and mercury concentrations in DRC rivers near copper-cobalt and gold mining sites that exceeded the country's own legal limits for mine water discharge. A 2024 RAID and AFREWATCH report consolidated 22 scientific studies and 20 civil society reports confirming that rivers, lakes, streams, and groundwater near the DRC's mines are severely contaminated with arsenic, lead, mercury, cadmium, uranium, and acidic pollutants. More recently, a November 2025 dam collapse at a Chinese-operated cobalt mine in Haut-Katanga Province released acidic water laden with lead and arsenic directly into community wells and waterways. For communities living and working in these mining regions, acute and chronic arsenic toxicity is a proximal environmental hazard.
Browse Products from Our Shop









The Diagnostic Gap
Despite the documented environmental reality of heavy metal contamination, diagnostic efforts in the region rely almost exclusively on identifying viral pathogens. Reports indicate that of 500-plus suspected cases in a given outbreak cluster, only 50 or so individuals may actually undergo genomic sequencing (and zero received heavy metals testing). The current Bundibugyo outbreak in eastern DRC is suspected to involve more than 906 cases and 223 deaths, with the World Health Organization warning that the toll is likely to rise, yet only a fraction of these cases are receiving laboratory workup to confirm presence of ebolavirus. Every person who presents with these severe symptoms at a hospital in the Congo should be receiving a comprehensive screening, including a urinary or blood arsenic test, but they are not.
It is important to examine the inherent limitations of the technologies currently used to define these outbreaks. Genomic sequencing simply identifies the presence of specific genetic material; it does not inherently prove that the detected virus is the active cause of the patient's acute disease state. An individual can harbor viral material in their system without an active, causative infection.
Similarly, Polymerase Chain Reaction (PCR) testing is functionally misunderstood in broad public health applications. Kary Mullis, the 1993 Nobel Prize-winning inventor of the PCR technique, explicitly stated that PCR is a manufacturing process designed to amplify DNA sequences. In Mullis's own recorded words, PCR is "just a process that's used to make a whole lot of something out of something… It doesn't tell you that you're sick, it doesn't tell you that the thing you've ended up with really was going to hurt you or anything like that." It is not reliable on its own for determining the clinical cause of a disease. Amplifying a fragment of genetic material does not equate to isolating an infectious agent or proving that the detected material is the root cause of the symptoms presented.
Kary Mullis, recipient of the 1993 Nobel Prize in Chemistry for his invention of the polymerase chain reaction (PCR) technique. Image courtesy of The Nobel Prize.
Pharmaceutical Focus vs. Root Cause Investigation
While fundamental environmental toxicology is largely bypassed, global health initiatives are heavily invested ($$$$) in the rapid development of pharmaceutical countermeasures. As of June 1, 2026, the Coalition for Epidemic Preparedness Innovations (CEPI) announced approximately $60 million in fast-tracked funding toward three Bundibugyo ebolavirus vaccine candidates. The breakdown includes up to $50 million to Moderna for an mRNA-based candidate, up to $8.6 million to the University of Oxford (with manufacturing by the Serum Institute of India) for the ChAdOx1 BDBV candidate (which uses the same viral-vector platform as the Oxford/AstraZeneca COVID-19 vaccine), and an initial $3.2 million to the International AIDS Vaccine Initiative (IAVI) for an rVSV-based candidate.
While high-tech pharmaceutical development commands vast resources and accelerated regulatory timelines, basic, life-saving diagnostic logic is being skipped/overlooked (I wonder why that is?).
A Question of Public Health
If the primary goal of public health is to save lives through precise and accurate treatment, the differential diagnosis must also include all probable local hazards. Ruling out heavy metal toxicity is a necessary first-principles step to ensure that afflicted individuals receive the correct care, particularly because the treatment protocols differ dramatically. Viral hemorrhagic fever is managed with supportive care, fluid replacement, and experimental antivirals or monoclonal antibodies. Acute arsenic poisoning, by contrast, is treated with chelation therapy using agents like dimercaprol or DMSA (succimer), alongside aggressive fluid and electrolyte management. A patient suffering from acute heavy metal toxicity who is presumed to have a viral infection will not receive the antidote they need.
This prompts a vital question: Why aren't we performing a very cheap and easy-to-administer test to narrow the differential diagnosis and eliminate acute arsenic poisoning in an area where local gold mines make it a highly likely possible root cause?
Sources and Further Reading
The following sources informed this article and offer additional depth for readers interested in the science, the regional environmental context, and the current outbreak response.
- Myango M, Pascal M, Wivine M, Bahananga M, Katcho K. "Insights into trace metal(loids) contamination in mining and agricultural soils of the Democratic Republic of Congo: A systematic review." ScienceDirect.
- Muimba-Kankolongo A, Banza Lubaba Nkulu C, Mwitwa J, Kampemba FM, Mulele Nabuyanda M. "Impacts of Trace Metals Pollution of Water, Food Crops, and Ambient Air on Population Health in Zambia and the DR Congo." Journal of Environmental and Public Health, 2022. (PMID: 35844936; PMCID: PMC9277192.)
- "Protecting Miners' Health in the Democratic Republic of Congo." Think Global Health.
- International Journal of Toxicology and Risk Assessment. ClinMed Journals.
- "Pollution causing birth defects in children of DRC cobalt miners, study finds." The Guardian, May 6, 2020.
- "Contamination by heavy metals from mining activities: An ecological impact assessment of Mura and Kimpulande Rivers, Democratic Republic of the Congo." Environmental Advances, 2022.
- "The Road to Ruin: Environmental Pollution and Human Costs of the DRC's Cobalt Boom." RAID and AFREWATCH, 2024.
- "DR Congo suspends Chinese cobalt miner after Lubumbashi chemical spill." Semafor, November 10, 2025.
- "Medical Management Guidelines for Arsenic Trioxide." Agency for Toxic Substances and Disease Registry (ATSDR), CDC.
- "Arsenic Toxicity: Clinical Assessment." ATSDR Environmental Medicine Case Study, CDC.
- "Acute arsenic intoxication." PubMed clinical review.
- "Arsenic Toxicity." StatPearls, NIH National Library of Medicine.
- "Arsenic Poisoning: Causes, Symptoms and Treatment." Cleveland Clinic.
- "Ebola Disease Fact Sheet." World Health Organization.
- "Ebola Disease Basics." Centers for Disease Control and Prevention.
- "Ebola." Johns Hopkins Medicine.
- "Experts convened by WHO advise on candidate treatments and vaccines for Ebola disease caused by Bundibugyo virus." World Health Organization, May 28, 2026.
- "CEPI fast-tracks three Bundibugyo ebolavirus vaccine candidates." Coalition for Epidemic Preparedness Innovations, June 1, 2026.
- "Statement on vaccine efforts relating to the Bundibugyo Ebolavirus outbreak in the DRC." University of Oxford, May 22, 2026.
- "Vaccines for Bundibugyo Ebola virus outbreak are being developed, but none are ready yet." Scientific American.
- "Dimercaprol Injection." MedlinePlus, U.S. National Library of Medicine.
- "Succimer (DMSA)." MedlinePlus, U.S. National Library of Medicine.